Below I have tried to summarise my presentation to the Us in a Bus 30th Anniversary Conference (23.03.23). I started by quoting quantum physicist Niels Bohr who (allegedly) said that “the only thing I can’t predict … is the future!”. But I did set out some of the historical contexts prior to and during the development of Intensive Interaction so that I could extrapolate from there. Below I have adapted some material from the slides I used:
Before Intensive Interaction (BII):
(looking a bit at the historical context of education and care for people with learning disabilities that lead to the development of Intensive Interaction)
~ ‘Tender Loving Care’: prior to the Education (Handicapped Children) Act 1970 children with severe or profound learning difficulties were deemed ‘ineducable’. Also for many children and adults with severe or profound learning difficulties, life-long hospital ‘care’ (hopefully ‘tender’ and ‘loving’ – although not always) was often the norm, with little thought given to possible educational or psychological development.
~ Then came a ‘Stimulation’ phase that challenged the passivity of ‘TLC’ care, with activities developed to ‘stimulate’ the participants e.g. multi-sensory rooms, musical activities or ‘rebound’. However, people were still often engaged in activities they had not chosen and had little or no control over.
~ Next came the Behavioural phase, which attempted to structure activities for people in order to ‘improve’ or somehow change their behaviour. Thus, ‘teaching’ (and care) became outcome focused, with learning ‘programmes’ set for individuals. But again such programmes were not chosen by the people themselves, but were applied to them by others around them.
~ Then came a ‘Person-centred’ or ‘Responsive’ Phase: this phase looked to differentiate activities and services provided for people on an individualised basis (in theory) building on their strengths and personal preferences … and is perhaps best evidenced in the development of approaches like … Intensive Interaction.
(the above is adapted and developed from the work of SLT Cath Irvine in Understanding Intensive Interaction: context and concepts for professionals and families (JKP; 2010, p. 22-25))
The 1980s – the ‘development phase’ of Intensive Interaction:
In the 1980s some teachers became uneasy with behaviour modification techniques, and so consideration was then given to nurturing natural forms of communication and relationship building. The staff at Harperbury Hospital School, led by Dave Hewett and Melanie Nind, started to think about how to help their students further develop their ‘fundamental communication’ abilities. Dr Geraint Ephraim, a clinical psychologist, had developed an approach he called ‘augmented mothering’, and some of the Harperbury staff meet with Dr Ephraim who suggested they read up on infant-caregiver interactions.
By 1986 the Harperbury team felt their Intensive Interaction approach was well enough developed to be communicated to others, and in 1987 Melanie and Dave presented: ‘Interactive Approaches to the Education of Children with Severe Learning Difficulties’, at a conference at Westhill College in Birmingham, UK. In 1988 the first academic paper was published on Intensive Interaction (by Nind & Hewett, obs): ‘Interaction as Curriculum’ in the British Journal of Special Education. Then the practitioner-led dissemination of the approach began with Dave and Melanie being invited to speak at a number of conferences and to give talks and training sessions to staff teams across the UK.
The 1990s – The dissemination and research phase of Intensive interaction:
In the 1990s the dissemination of Intensive Interaction continues: the approach becomes increasingly practised in SEN schools in the UK, and starts to be recognised in some adult services. International interest was just starting, initially in the Netherlands. In 1994 the first book on Intensive Interaction was published: Access to Communication (Nind & Hewett, David Fulton). Also, the first outcomes-focused research begins to be published, including:
Watson, J. & Knight, C. (1991) ‘An evaluation of Intensive Interaction teaching with pupils with severe learning difficulties’, Child language, Teaching and Therapy, 7(3), 10-25.
Nind, M. (1996) ‘Efficacy of I.I.: developing sociability and communication in people with severe and complex learning difficulties…’, European Journal of SNE, 11(1), 48-66.
Watson, J. & Fisher A. (1997) ‘Evaluating the effectiveness of I.I. teaching with pupils with profound and complex learning difficulties’, British Journal of Special Education, 24(2), 80-87.
Lovell, D., Jones, R. & Ephraim, G. (1998) ‘The effect of I.I. on the sociability of a man with severe intellectual disabilities’, Int. J. of Practical Approaches to Disability, 22(2), 3-9.
From 2000-2010: there continues to be more Intensive Interaction dissemination and research:
In 2002 Dave Hewett and SLT Cath Irvine organised the first UK Intensive Interaction Conference, attended by well over 200 delegates at Birmingham University (I was there as well!). Then in 2002 the first Intensive Interaction training video ‘Learning the Language’ by Phoebe Caldwell, was released. In 2003 http://www.IntensiveInteraction.co.uk, the first Intensive Interaction website was launched. At an international level, in 2008 the first Australasian I.I. Conference was held in Brisbane hosted by Dr Mark Barber and Janee Williamson.
During this decade more outcome-focused research was published, including:
Kellett, M. (2000) ‘Sam’s story: evaluating Intensive interaction in terms of its effect on the social and communicative ability of a young child with severe learning difficulties’, Support for Learning, 15 (4), 165-71.
Elgie, S. & Maguire, N. (2001) ‘Intensive Interaction with a woman with multiple and profound disabilities: a case study’, Tizard Learning Disability Review, 6(3) p.18.
Leaning, B. and Watson T. (2006) ‘From the inside looking out – an Intensive Interaction group for people with profound and multiple learning disabilities’, British Journal of Learning Disabilities, 34, 103-109.
From 2000-2010 – but the research focus begins to broaden
During this time the research and published literature supporting Intensive Interaction began to open up in terms of there being a broader focus, apart from just outcome-focused research. Such a change is perhaps best illustrated by the following papers:
Cameron, L. & Bell, D. (2001) ‘Enhanced Interaction Training: A method of multi-disciplinary staff training in Intensive Interaction to reduce challenging behaviour in adults…’, Working with People who have a Learning Disability, 18(3), 8-15.
Culham, A. (2004) ‘Getting in Touch with our Feminine Sides? Men’s Difficulties and Concerns with Doing Intensive Interaction’, BJ of Sp. Ed., 31(2), 81- 88.
Barber M. (2007) ‘Imitation, interaction and dialogue using Intensive Interaction: tea party rules’, Support for Learning, 22: p.124–30.
Firth, G., Elford, H., Leeming, C. & Crabbe, M. (2008) ‘Intensive Interaction as a Novel Approach in Social Care: Care Staff’s Views on the Practice Change Process’, Journal of Applied Research in Intellectual Disabilities, 21, 58-69.
Samuel, J., Nind, M., Volans, A. & Scriven, I. (2008) ‘An evaluation of Intensive Interaction in community living settings for adults with profound intellectual disabilities’ Journal of Intellectual Disabilities, 12(2), 111-126.
Zeedyk, S., Davies, C., Parry, S. & Caldwell, P. (2009) ‘Fostering social engagement in Romanian children with communicative impairments: The experiences of newly trained practitioners of Intensive Interaction’, BJ of L.D., 37(3), 186-196.
From 2010 onwards: the use of Intensive Interaction broadens across user groups, practitioner groups, service or care contexts and location
Moving into the present, Intensive Interaction has now vastly expanded out from its original classroom (at Harperbury Hospital School) to many other schools and colleges (special and mainstream), and is used in families, in residential services, in day services, in hospitals, in care homes, by teachers and support staff, by parents and family members, by speech therapy services, by occupational therapy, in psychological services, etc, etc, etc. (Rogers & Hammerstein, 1951).
The approach is now also used across a wide range of groups of people with social or communication difficulties, be it because of an intellectual disability, or autism, or dementia, or Acquired Brain Injury, or challenging behaviour (due to communication breakdown), or children with PDA, or more recently PDOC/MCS. It is also now used across the world e.g. in the UK, Australia, Denmark, the Caribbean, Finland, South Africa, France, Germany, Russia, Greece, Romania, Moldova, Thailand, Malaysia, Brazil, Spain, USA, and many other countries besides.
Also, the approach is now taught on a variety of professional qualifications, at both undergrad and post-grad level, including: SLT, OT, DClin psychology, SEN teaching, early years, social work, disability studies, LD nursing, etc, etc, etc. (Ibid). Intensive Interaction is also now explicitly advocated in Government and NGO practice guidelines, in the UK from the Dept. Health, the Dept of Ed & Science, the RCSLT, the RCP/BPS, NICE (in everything but name), etc, etc, etc. (Ibid).
Also, the Intensive Interaction research focus has become much broader and has begun to differentiate in the user group and context of use, and is sometimes used alongside or integrated into other approaches e.g.:
Fraser, C. (2011) Can adults on the autism spectrum be affected positively by the use of intensive interaction in supported living services? GAP, 12 (2), 37-42.
Ellis, M. & Astell, A. (2011) Adaptive Interaction: a new approach to communicating with people with advanced dementia. Journal of Dementia Care, 19(3), 24-26.
Berry, R., Firth, G., Leeming, C. & Sharma, V. (2014) Clinical Psychologists’ Views of Intensive Interaction as an Intervention in Learning Disability Services, Clinical Psychology & Psychotherapy, 21(5), 403-410.
Tee, A. & Reed, R. (2017) Controlled study of the impact on child behaviour problems of Intensive Interaction for children with ASD, Journal of Research in Sp. Educational Needs, 17(3), 179-186.
McKim, J. & Samuel, J. (2020) The use of Intensive Interaction within a Positive Behaviour Support framework, British Journal of Learning Disabilities, 49(2), 129–137.
Strange, J. (2021) Improvised music to support Intensive Interaction for children with complex needs: A feasibility study of brief adjunctive music therapy, British Journal of Music Therapy, 35 (2), 43–52.
Berridge, S. & Hutchinson, N. (2021) Mothers’ experience of Intensive Interaction, Journal of Intellectual Disabilities, 26 (2), 391–406.
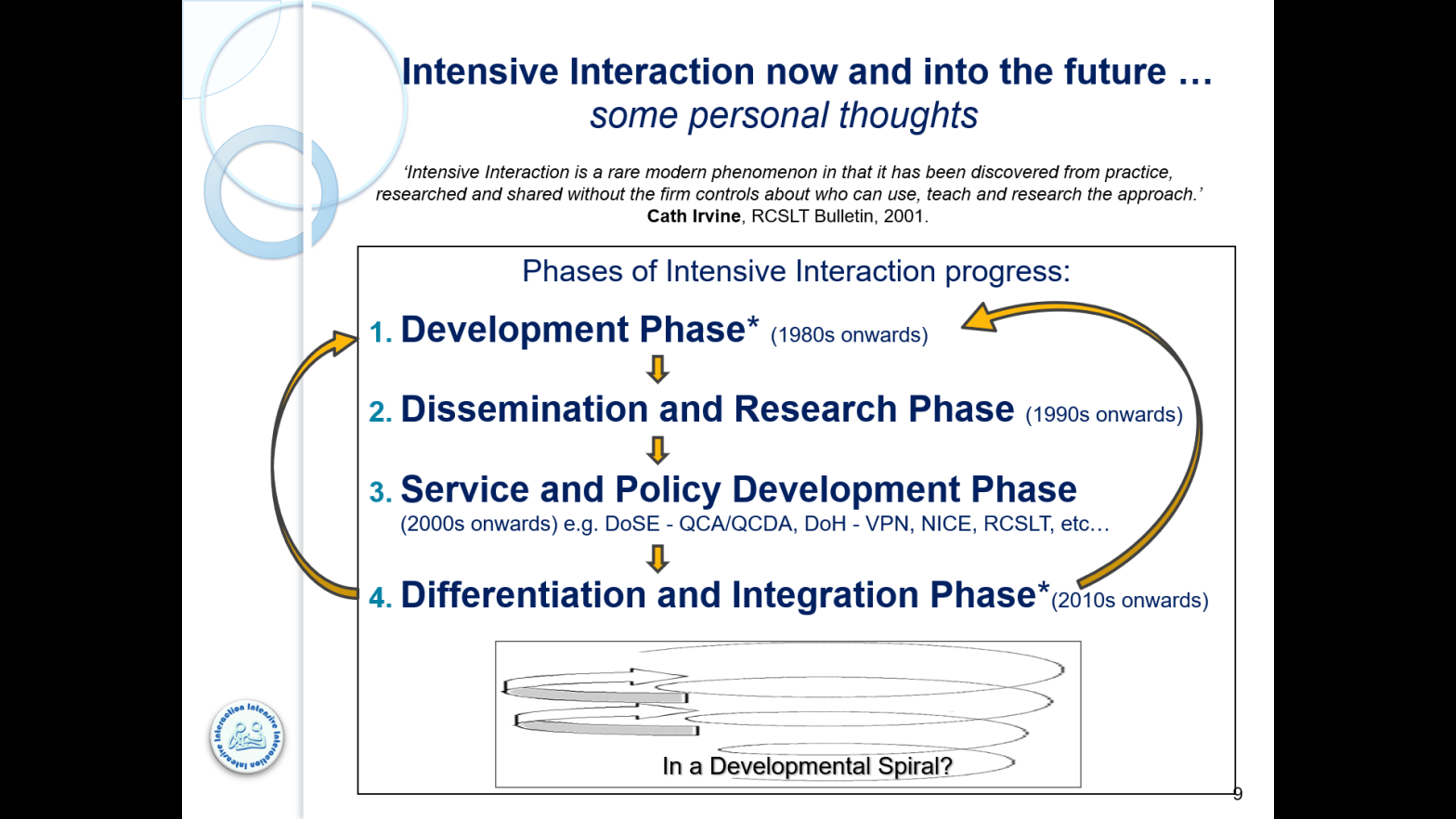
So, from all this history over the past 30 or so years, I think that there are also distinct phases of Intensive Interaction development, which I tried to sum up and visually illustrate in this diagram:
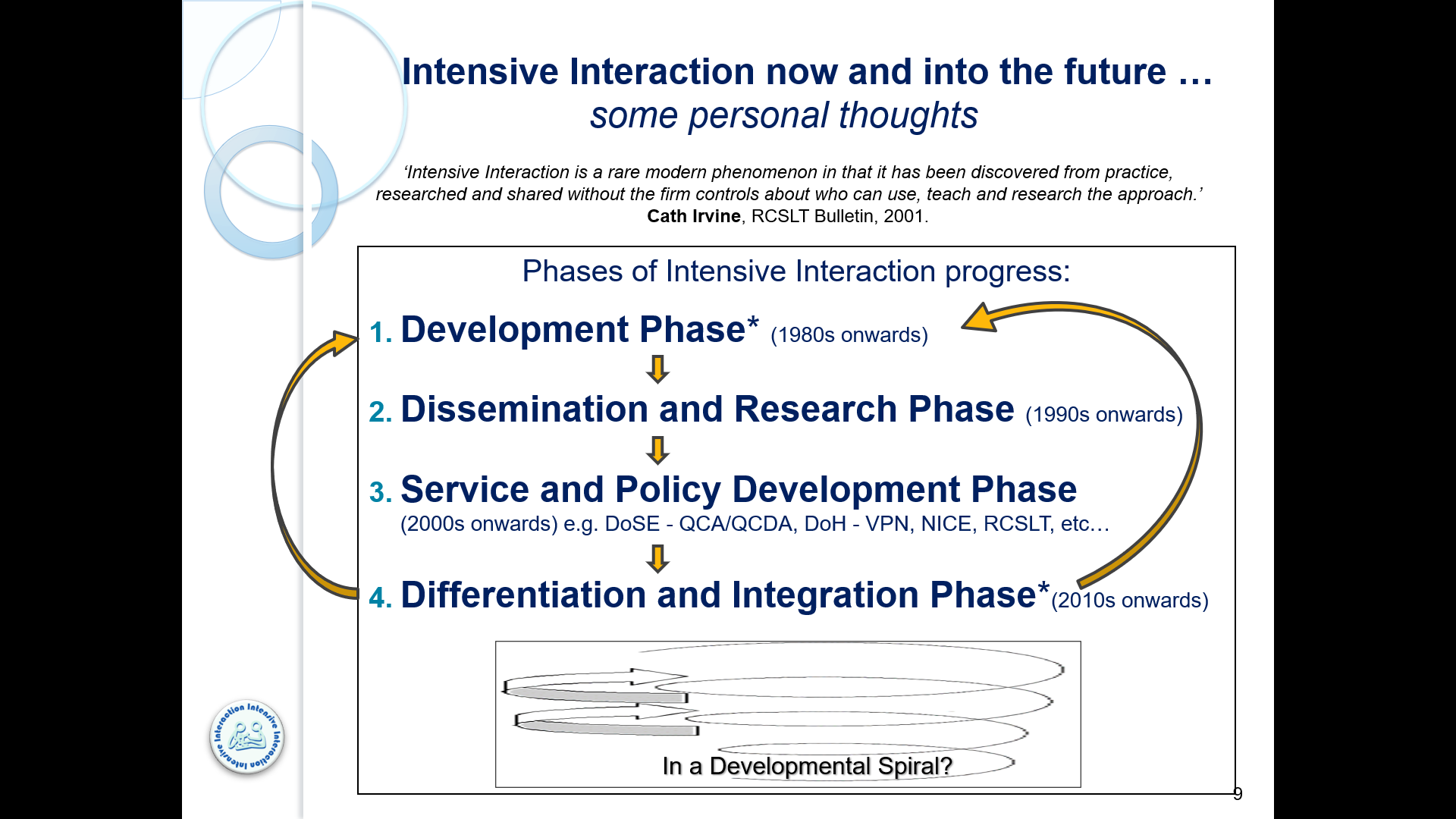
My conclusions, after looking back at its journey into the present context of multiple uses, are that Intensive Interaction has already started to become differentiated by its application with different service user groups across an ever wider range of care, educational or therapeutic contexts (as noted above).
But interestingly Intensive Interaction is also now more and more integrated into other more holistic approaches to care, support and/or education e.g. by being used alongside or integrated into other approaches or care frameworks e.g. sensory processing support or music therapy, or as a proactive strategy within a Positive Behaviour Support framework.
I also feel that this broadening of its differentiated or integrated application should feed back into our general understanding of the utility and application of the approach as a whole, and therefore add more nuanced understandings back into a further, secondary developmental phase that can then again be disseminated and again go on to inform practice and future service and policy development – a bit like a developmental spiral (a model taken from the development of Intensive interaction itself!). Well, blow me down!
In a future Blog I will offer some thoughts on the potential ‘Pros and Cons’ of such a ‘Differentiation and Integration Phase‘ of the Intensive Interaction journey – but please feel free to add your own interpretation of, or thoughts about, this model in the ‘Comments’ section (somewhere below).

Thanks Graham. Great to have the summary of research here, alongside your insight into the journey.
LikeLiked by 1 person
Would have loved to have been there and heard and seen all of the presentations and conversations. I’d love to hear more about the differentiation and integration. I have been thinking more about II as a form of accessible language for some people. In my thinking, my mantra, “how do I need to be in order to be with you?”, the answer, for some individuals, undoubtedly is to communicate in means and through a lens of II. For other individuals, the means and lens may be different… would this be consistent with your thinking about differentiation… or am I off track?
LikeLiked by 1 person
Hi Sheri,
I will expand on my definitions of ‘differentiation’ and ‘integration’ in a follow-up Blog in a couple of week’s time – however, your question “how do I need to be in order to be with you?” is sort of central to the issue, because (I think) that Intensive Interaction as practiced by many people is different in both form and context with different people who are are at times quite radically different in their personal, physical and sensory characteristics, and in their available communication means and sociability (and therefore is in some way always differentiated when used across radically different recipient groups) ; one example being the Adaptive Interaction approach set out by Maggie Ellis and Arlene Estelle. However, any differentiation in or of the form and context of such intensive interactivity will still need to remain true to the central principles of the original II approach as set out in the original literature. But whether we like it or not there are differences (e.g. between II being seen and used as part of a school pedagogy and curriculum for SEN Children, and care staff ‘hanging out’ with adult residential or day service folk, or it being used with people with advanced dementia … and I think it would be best if we somehow got ahead of the game (because it is already happening) and try to think through the consequences of this potential movement away from a more generic view of II being held by an already established community of practice.
LikeLike
Great summary GF. Having reflected on the route that I I. progressed in relation to its historical context, it would be interesting to read your idea of the contexts that the Institute hopes to have influence in in the next decade or so and hiw it will go about achieving that
LikeLiked by 1 person
Hi Mark,
Good point – can we (as an Institute) get ahead of the game on this (because I think that it is already happening) and try to think through the consequences of this potential movement away from a more generic view of II being held, defined and developed by an already established community of practice. In answer to your point about how the II Institute might hope to have influence in this area in the next decade … I’m not sure, as I haven’t talked to anyone from the Institute yet about this idea (I only really formalised it in my own mind in the week or so before the Us in a Bus Conference), and I still need more time to think more about the Pros and Cons of this myself (I think). But everyone else’s views on this would be most welcome!
LikeLike
HI Graham,
What a lovely pathway for II to have taken. Brilliant drive by yourself and your colleagues/peers as well as others around the world to apply this. As an adult social care worker with a background in PBS (but an awareness of its limitations and frailities), II has interested me from a perspective (Adults only) or its place in the outcomes of Wellbeing (improvements), sence of belonging/attunement, rapport development, enabling a feeling of safety in a chaotic world, hanging out tool and application of more MoQ’s (moments of quality)……. as well as trauma recovery tool, mode of showing respect/dignity and finally a ‘talking’ therapy for someone who either doesn’t want to talk or communicates in a neurodivergent way.
My wonder is the place of II’s future for ‘adults’ being in those areas above forward and formalising them as a focus/outcome of II. As a community interest company (that is undertaking a journey towards being a Trauma Informed Care provider), we have addapted ‘A Framework for Recognising Progression In Intensive Interaction’ to include one for adults that we call ‘A Framework for therapeutic support around MoQ, belonging, attunement, trauma recovery and rapport’ whereby we view this as being the point of II.
We don’t have the evidence to support this, but, i feel strongly that our application of II has resulted in an holistic theraputic rapport for one young man wihtout the drive of childrens based II – the drive purely being to enable an increased sence of safety. I watched some of the clips of II from the conference last year and saw how II was being encourperated in to PBS model, but, i am not sure this is the right direction as i would hope it can become an additional element towards the emotional context that embodies wellbeing as a primary startergy, secondary stratergy, setting event and reactive stratergy for positive emotions and support with negaitve emotions.
i would love to connect more about this.
Loving your work
LikeLiked by 1 person
Your work is sounding great too Luke. Would love to see more of your Framework, putting front and centre the human needs of people supported.
LikeLike
Great to refresh myself of the content of this. Thank you. As always, a mixture of despair and positivity are my over riding feelings post conference🤷🏻
LikeLike